
Ebola emergency
Despite major efforts to scale up the Ebola disease outbreak response in Democratic Republic of Congo (DRC), the situation remains a significant public health emergency as the virus continues to spread to new areas and international support falls well short of what is needed.
MSF staff are leading experts in treating and containing Ebola. Our teams worked tirelessly throughout the massive 2014 to 2016 West Africa epidemic and have responded to multiple outbreaks in DRC alone.
As of July 6, there have been 1,708 confirmed cases, 580 confirmed deaths and 280 survivors since the Ebola disease outbreak was declared on May 15, 2026. There have also been 20 confirmed cases in nearby Uganda. The outbreak’s epicentre remains in DRC’s eastern province of Ituri but is spreading into new areas.
Unlike most previous Ebola disease outbreaks, this outbreak is caused by the Bundibugyo virus. It kills up to 40 per cent of people infected, making it less lethal than the more common Ebola virus.
However, there is currently no approved vaccine and no approved treatment, so responding to this virus has been particularly challenging. The evolving situation, coupled with the growing concern that people are reticent to seek care away from their homes, means Ebola care must be decentralized outside of main urban centres.
In early July, the World Health Organization (WHO) began sponsoring a clinical trial to identify effective treatments. The trial is being conducted in collaboration with many international research, clinical and humanitarian organizations, including MSF.
HOW CAN I HELP MSF?
Right now, our teams are responding in DRC. Donate now to help MSF medical teams act fast and support people facing emergencies around the world.



The latest: How is MSF responding to the Ebola disease outbreak?
MSF is running Ebola Treatment Centres across affected areas in Ituri and North Kivu, and South Kivu.
By July 3, 843 patients were admitted to MSF’s Ebola Treatment Centres in Ituri, North Kivu and South Kivu, including 357 confirmed Ebola-cases. There have been 116 survivors.
It is important to note that the Ebola disease outbreak is not the only health emergency that communities are facing in DRC. Essential services such as vaccination, maternal health, sexual and reproductive healthcare, nutrition, care for survivors of sexual violence, treatment for infectious diseases and other urgent medical needs must also continue.
MSF teams are often among the first humanitarian responders for one key reason: because we are already there. MSF has been working in DRC since 1977, providing vital healthcare services through conflict, disaster and disease.
Right now, we have hundreds of staff responding to the outbreak in eastern DRC. However, with little or no support from humanitarian actors outside of urban areas, and with the outbreak continuing to spread, MSF is concerned it will soon reach its maximum response capacity.

- More than 600 MSF staff are directly responding to the Ebola disease outbreak in DRC, working alongside Ministry of Health (MoH) teams. They are supported by more than 2,700 MSF staff, and nearly 4,500 incentivized MoH staff already working in the country on existing health programs, helping ensure that other essential health services continue. In Uganda, MSF has 20 staff responding to the outbreakThe response, led by the Congolese Ministry of Health and supported by several international partners, is expanding but still falls short of what is needed as the outbreak keeps spreading to new areas
- The outbreak is currently centred in Ituri, with the main epicentre around Bunia, Mongbwalu, Rwampara and Nyankunde health zones. However, other areas – outside of urban ones – show either none or little support by humanitarian actors
- Despite the recent scale up in efforts, MSF is still seeing critical gaps in response capacity, including in surveillance, testing, community engagement and rapid case detection
- MSF staff with experience responding to Ebola disease outbreaks continue being sent to DRC to as part of the emergency response. They will provide support to existing medical projects and respond to new alerts in surrounding areas
- MSF works to ensure strict infection prevention measures are in place for healthcare projects and facilities in DRC. We must protect patients and staff and ensure they can continue to access medical services
- MSF’s Ebola response is based on six pillars: caring for and isolating patients; tracing and follow-up of patient contacts; raising community awareness of the disease (such as how to prevent it and where to seek care); conducting safe burials; proactively detecting new cases; and supporting existing health facilities.

What is Ebola disease?
Ebola is a rare but deadly disease which can kill up to 90 per cent of those infected.
The most commonly known viruses within the Ebola disease genus are the Ebola virus, the Sudan virus and the Bundibugyo virus. There is an approved treatment and a preventive vaccine for the Ebola virus. But the current Ebola disease outbreak reported in DRC is caused by the Bundibugyo virus, for which there is no approved vaccine or treatment.
It can be difficult to diagnose because the early symptoms, like a fever and sore throat, are common. To confirm an Ebola disease diagnosis, special tests need to be carried out. These require test kits specific not to the disease itself, but to each individual virus in order to detect it. However, these test kits are currently in short supply for the Bundibugyo virus, which significantly slows down case confirmation and, consequently, the implementation of contact tracing and patient isolation.
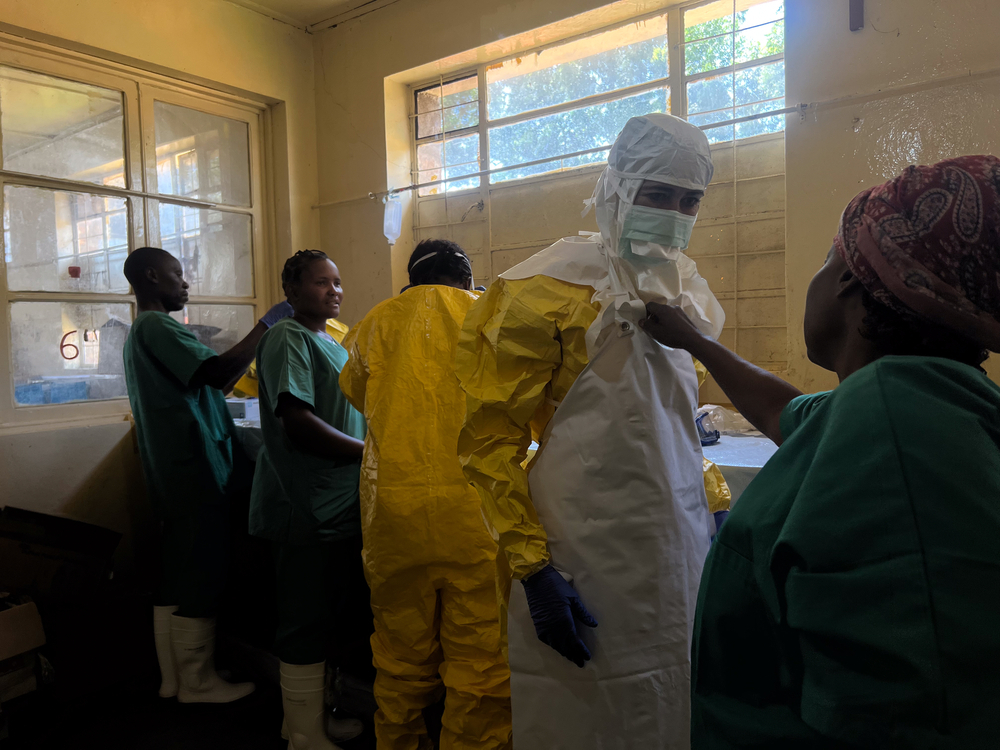
Ebola disease is highly infectious and can be transmitted from both animals and humans. Human-to-human transmission happens through close contact with blood, secretions or other bodily fluids of infected individuals. This is why people have to wear full personal protective equipment to prevent catching or spreading the virus.
Medical teams can give patients the best chance of survival by helping to manage the symptoms of the virus and treating other diseases the patient may have.
Once a patient recovers from Ebola disease, they’re immune to the form of the virus they contracted.
MSF’S response to Ebola in the West Africa
Between late 2013 and 2016, an outbreak of Ebola in West Africa became a major international emergency. The severity of the epidemic saw MSF launch one of the largest emergency operations in our history.
MSF responded in the three most affected countries — Guinea, Sierra Leone and Liberia — and also to the spread of cases to Nigeria, Senegal and Mali.
At the peak of the epidemic, MSF employed nearly 4,000 local medical staff and more than 325 international staff who ran Ebola treatment centres, as well as conducted surveillance, contact tracing, health promotion and provided psychological support.
MSF admitted 10,310 patients to our Ebola management centres, of which 5,201 were confirmed Ebola cases, representing one-third of all WHO-confirmed cases.
Myths & Truths About Ebola Disease (Bundibugyo virus)
| Myth | Truth |
| There is no point going to a treatment centre if there is no specific cure. | Even though there is currently no approved vaccine or specific treatment for Ebola caused by the Bundibugyo virus, treatment centres provide essential supportive care. This includes fluids, oxygen, nutrition and symptoms relief such as fever, vomiting, diarrhea and pain. This care helps the body fight the infection and improves the chances of survival. |
| If I am isolated, it means I already have Ebola disease. | Isolation is not a confirmation of disease. It is a precautionary step while tests are being done, because early symptoms of Ebola disease can look like other illnesses such as malaria or typhoid. Once results are available, isolation can be adapted depending on the diagnosis. |
| I only have mild symptoms, so I don’t need to go to a treatment centre. | Common symptoms like fever, headache, vomiting or diarrhea can mimic malaria, flu or typhoid. During an Ebola outbreak, it’s important to isolate and get tested to rule out Ebola disease, even if the chance is low. Early assessment and temporary isolation help protect you, your family, healthcare workers and the community. Getting checked early is always the safest choice. |
| If I am in a treatment centre, I cannot see or speak to my family. | Treatment centres are organized to maintain safe communication between patients and families. Whenever possible, patients can communicate through safe visiting areas or other communication tools. Maintaining family connection is part of overall care and wellbeing. |
| Doctors will use experimental drugs on patients without consent. | Although clinical trials began in early July, they are strictly regulated. These trials have been approved by international medical and ethical authorities and are conducted in close collaboration with health authorities. Participation in these trials remains strictly free and voluntary. Each patient receives clear explanations before making a decision. Refusing to participate would in no way affect access to standard medical care. |
| Ebola disease outbreaks are used for business or profit. | Ebola disease is a rare and highly dangerous illness that requires a fast and large-scale medical response to save lives and prevent further transmission. Because of this urgency, international health institutions mobilize quickly. This is not driven by profit, but by the need to respond effectively to a serious public health emergency. MSF uses our funding exclusively for medical and humanitarian activities – during Ebola outbreaks and beyond – including providing care for other essential health needs such as malaria, maternal health and pediatric services. |





