COVID-19 in West Africa: Focus on the most vulnerable and learning from the past
As of March 26, 2020, 43 out of 54 countries on the African continent are affected by the coronavirus pandemic. Sierra Leone remains the only countries to not register covid cases in West and Central Africa. Burkina Faso, Senegal, Cameroon, which are among the ones with highest number of cases in the region, have already moved to a stage of local transmission and are differently prepared to respond. Dr Dorian Job, Doctors Without Borders/Médecins Sans Frontières (MSF) West Africa Program Manager in Dakar, provides an update on the situation and priorities at this stage.
With the rapid spread of the coronavirus epidemic in recent weeks, the issue of the level of preparedness of African countries has been in the headlines of the international press. But one should wonder, which country was really prepared? Let’s look at the situation in Europe today, especially in countries like Italy, France and Spain, which one of them was prepared to face such a time bomb?
One also wonders whether the Ebola epidemic that affected West Africa between 2014 and 2016 has helped countries to be better prepared. This allowed at least the development of surveillance and coordination reflexes and mechanisms. It’s now just a matter of time to see how effective they were. Yet, in the meantime, we should already get prepared for the next phase, when the chains of contamination are no longer controlled and we have many more cases to deal with.
Most countries have already taken today measures to stop the spread of the epidemic (such as closing aerial borders, banning gatherings, closing schools) – without going as far as total confinement for the moment.
If they make it possible to slow the spread of the virus, these measures will however affect economies of countries and populations that often live from day to day. They will also impact on particularly vulnerable populations in the context of humanitarian crises.
Preventative actions in West African context
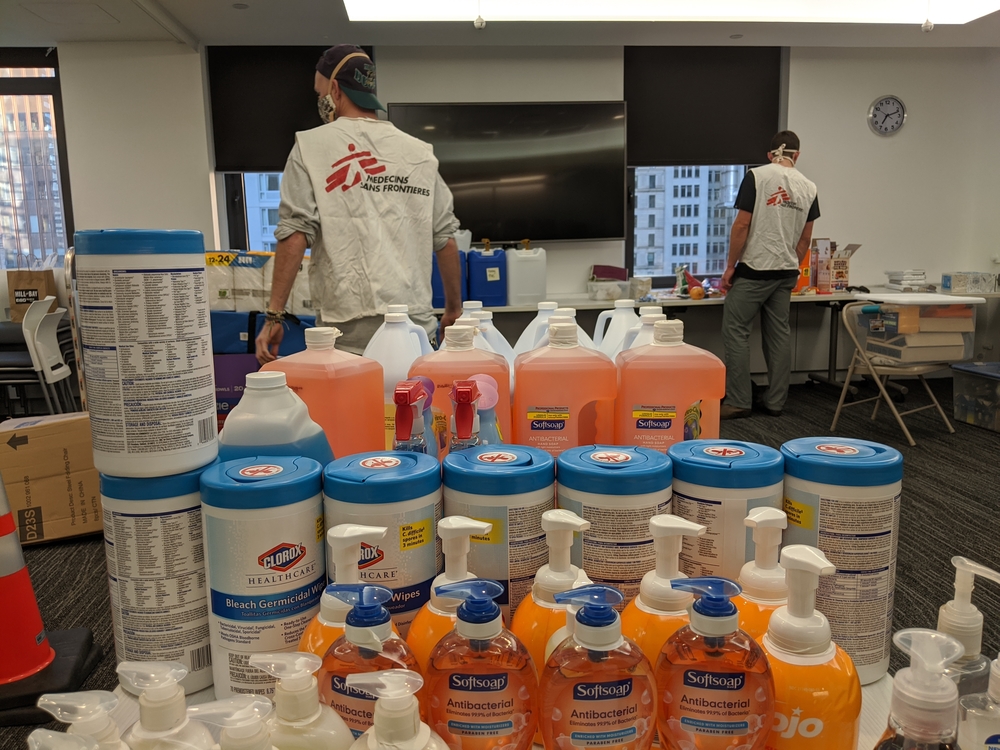
In Burkina Faso, for instance, it will be very difficult for all actors to ramp up the humanitarian response, as we were all calling for in response to insecurity and population displacements. None of us is today in a position to bring in new teams, and the medical supply system will be disrupted for weeks or even months. Yet, it’s not only imperative to strengthen the response to the humanitarian crisis, but more attention will have to be paid now to hygiene and infection prevention measures, in order to avoid any propagation of the virus, in a country where access to water is largely insufficient in distressed areas.
Each country will certainly have to adapt these measures soon, in order to balance between the necessary slowdown in the spread of the virus and the economic and social impacts that are likely to have.
Nevertheless, certain constants must remain regardless of the context.
First of all, what will make the difference in slowing down the epidemic is a change in individual attitudes: the respect for the 1.5 meters of physical distance we are told about and the application of basic individual hygiene measures.
Another key element in dealing with the epidemics will be our ability to identify, monitor and care for those most at risk, particularly in the communities. Coronavirus is a respiratory disease with a mild or moderate form for the vast majority, but it causes quite serious complications for those at risk, especially the elderly and people with other medical conditions. But we still know very little about its transmission in tropical areas or the consequences of co-infection with other chronic diseases such as diabetes or hypertension, or with more seasonal diseases such as malaria or malnutrition.
Non-coronavirus health threats
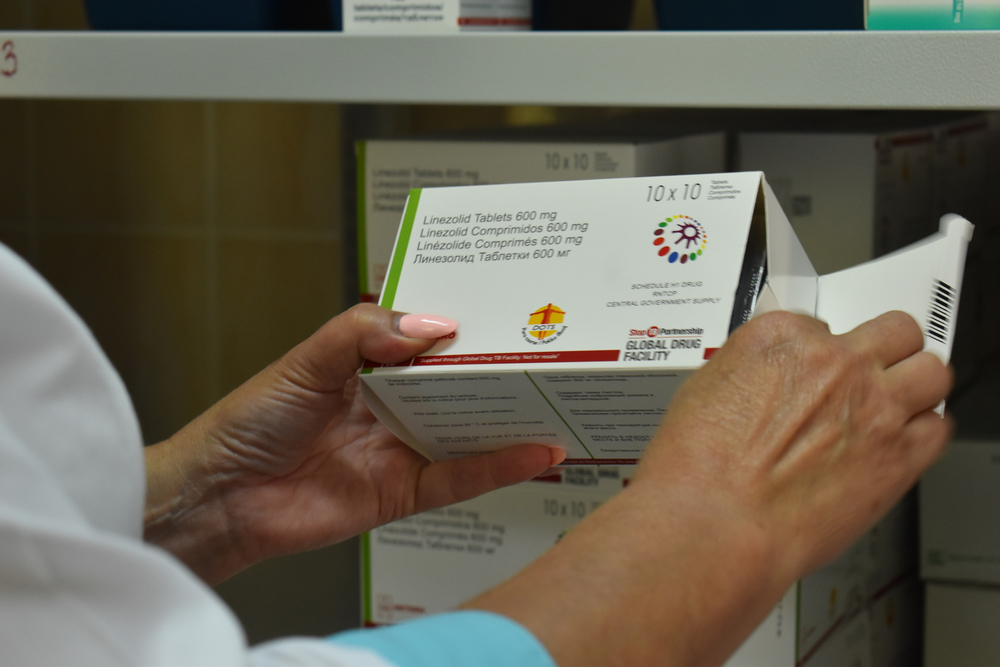
Finding an alternative to screening is also key, as the testing and diagnostic capacities are not sufficient at the moment. We will have to set up detection mechanisms based on symptoms and to develop epidemiological monitoring and referral systems for the most critical cases as close to the communities as possible.
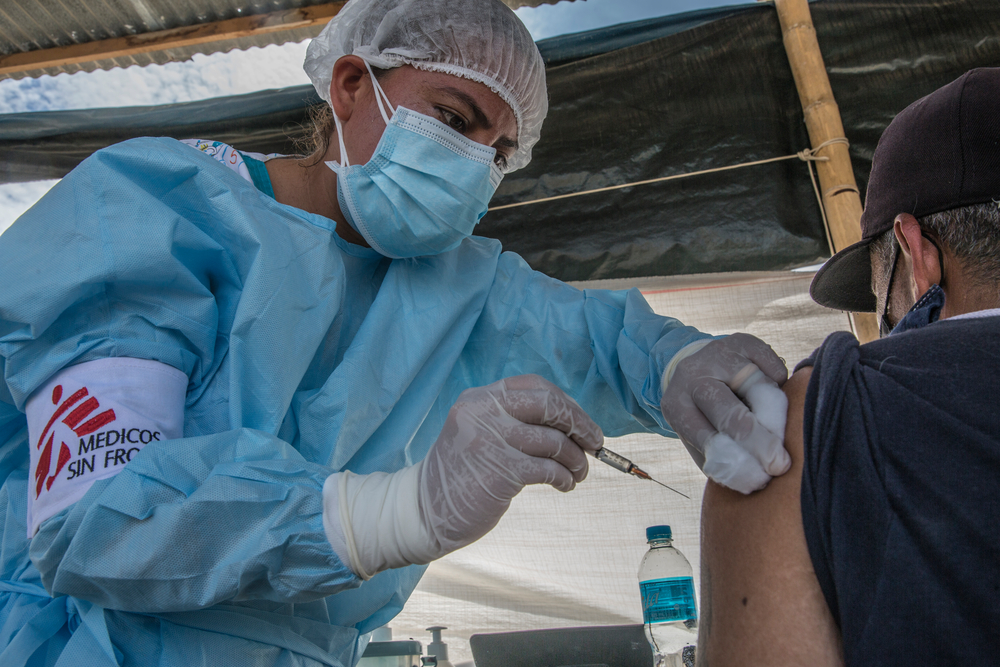
Nevertheless, the concentration of attention and energy on COVID-19 over the next few weeks may bring us to forget other health aspects and leave aside a large part of the population. As an example, malaria or measles – for which epidemic outbreaks have recently appeared in Burkina Faso or Niger – remain high mortality diseases in these countries and it’s necessary to carry out preventive activities or vaccination campaigns. Yet, we face the risk of not being able to deploy sufficient resources.
We have to draw lessons from past epidemics, including the Ebola experience in the region.
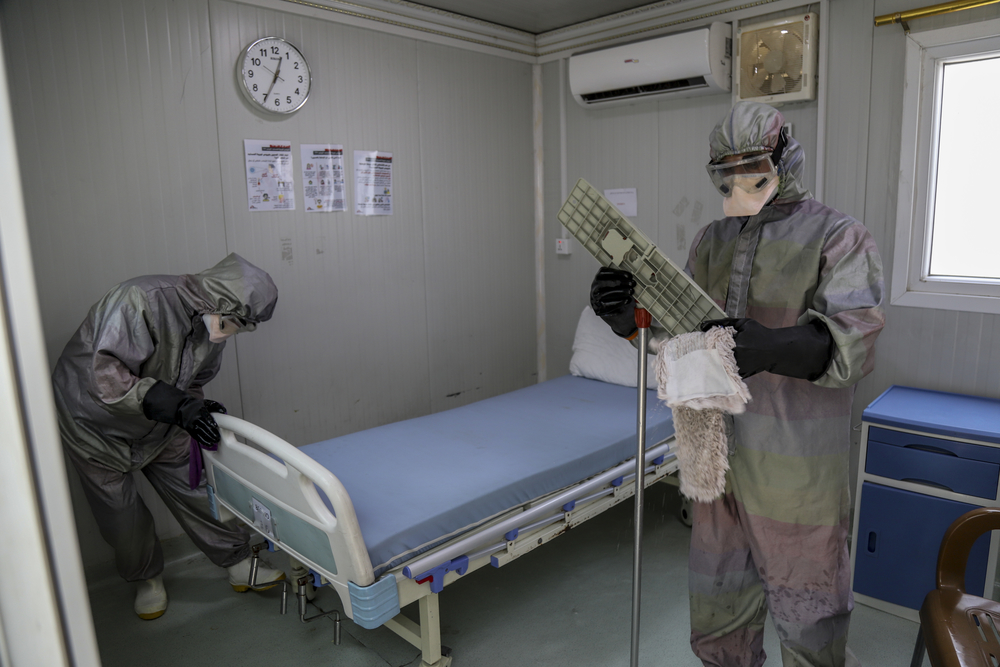
What we need to remind in priority: ensuring safety of health workers; maintaining confidence in the response and the actors implementing it, as it is essential to avoid panic and ensure the dissemination of the right information; not neglecting other patients.
At the same time, one must be also cautious to not simply reproduce all the elements of an Ebola response: i.e. putting in place, for example, Ebola-type protective measures (such as coveralls) for a virus that is not contagious through the skin. Let’s favour on the contrary decentralized care structures to manage simple cases and avoid the treatment centres being overwhelmed with simple cases (80%) that do not require hospitalization. Previous SARS experience also evidenced that well-ventilated structures with natural light offer much better infection control conditions than sophisticated structures with a closed air circuit.
In short, we’ll have to take stock of the past and innovate. I would not be surprised actually if new solutions for responding to this coronavirus epidemic come from the African continent. African countries have indeed more experience in managing health emergencies and public health reflexes are more developed there than in Europe: we are moving faster and easier towards simplifying medical protocols and standards, which could allow a quicker response in a situation like this.