Adapting our way of working and keeping essential medical services running during the COVID-19 pandemic
The impact of the COVID-19 pandemic has been felt in every one of Doctors Without Borders/Médecins Sans Frontières (MSF)’s approximately 450 projects in more than 70 countries. Since the beginning of the pandemic, MSF has had two main priorities: first, to keep existing essential medical services up and running for the hundreds of thousands of patients who rely on us; and second, to prepare for, and respond to the spread of the virus itself. Faced with challenges on a scale never experienced before, MSF’s teams, like frontline healthcare workers everywhere, have had to quickly adapt to the new realities of a COVID-19 world.
MSF has launched targeted COVID-19 projects in many of the countries hit hardest by the pandemic, including Italy, Spain, France, Belgium, Brazil and the US. At the same time, our teams around the world have been working to maintain MSF’s regular medical services, while preparing for the virus to hit the vulnerable communities we help – and all this at a time when lockdowns and travel bans are restricting the movement of medical staff and supplies.
“The challenges have been immense and we’ve adapted our entire way of working,” says Brice de le Vigne, head of MSF’s COVID-19 taskforce. “As a global humanitarian organization, our surge capacity during emergencies is normally built on being able to move specialist experienced staff and medical supplies around the world at a moment’s notice. But with travel restrictions, lockdowns and unprecedented disruptions in the global supply chain of essential personal protective equipment, medicines and medical materials, our teams have been pushed to find solutions beyond our usual way of operating to be able to continue caring for patients.”
Devastating knock-on effects
While the world’s attention is understandably focused on the direct impact of the COVID-19 pandemic, it is essential to see the health crisis from a broader perspective. In many of the places where MSF works – where health systems are already fragile and people often live in extremely precarious conditions – the indirect impact of the pandemic could be catastrophic.
“Getting the pandemic under control is clearly a priority for everyone, but it was never an option for us just to drop our regular medical services and focus solely on COVID-19,” says Kate White, medical focal point for MSF’s COVID-19 taskforce. “We know from decades of experience in other outbreaks that the knock-on effects on the rest of the health system can be just as, if not more, devastating than the disease itself. Keeping essential health services available and accessible is vital to prevent losing even more lives, whether from malaria, measles, malnutrition or complicated pregnancies.”
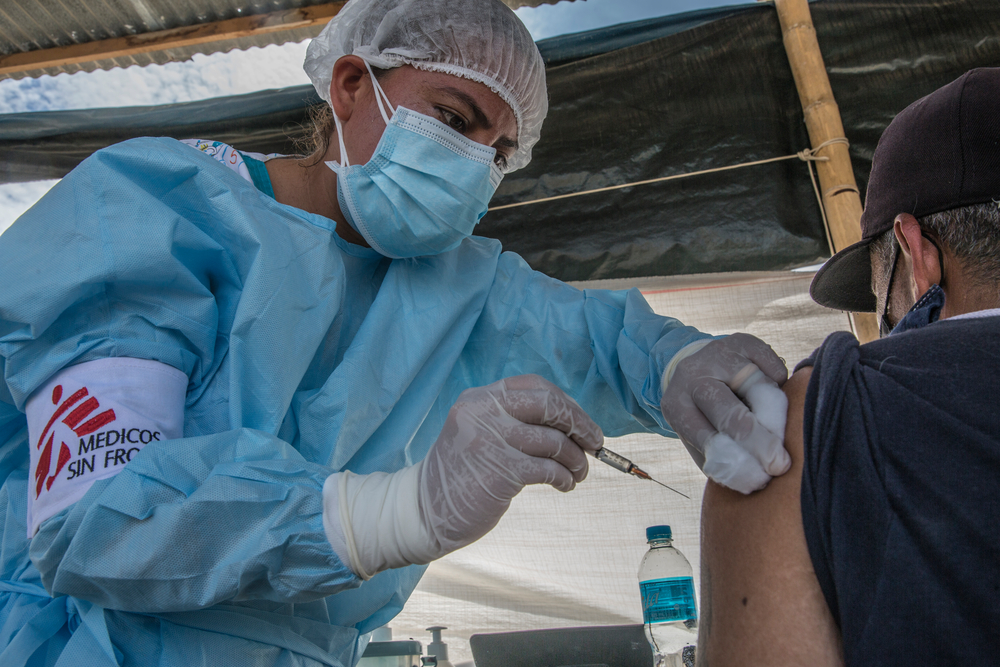
The COVID-19 pandemic risks further reducing vulnerable people’s already limited access to healthcare, as resources – both human and financial – get diverted from regular healthcare to the COVID-19 response. Health services may be downsized or closed to limit the risk of transmission, vital vaccination campaigns may be cancelled, while frontline healthcare workers may fall sick or die in places where there were already too few to go around.
Fear of infection
At the same time, people may put off seeing a doctor for any number of deadly medical conditions due to the difficulty of moving around during lockdowns or from fear of becoming infected with COVID-19 in a health facility. MSF teams have already seen a significant decrease in the number of patients coming to our facilities – in some cases by up to 50 percent – in projects in Bangladesh, Democratic Republic of Congo (DRC), Afghanistan, Nigeria, Sierra Leone and Egypt.
“The challenge for pregnant women is that no taxis or public service vehicles are operating after curfew, not even the boda boda [motorcycle taxis] that people use in informal settlements,” says George Wambugu, medical activities manager in Mathare, Kenya. “This leaves mothers exposed to obstetric complications. We recently had a mother deliver a pre-term baby in our ambulance who was in need of resuscitation. Luckily, the baby survived and both recovered well.”
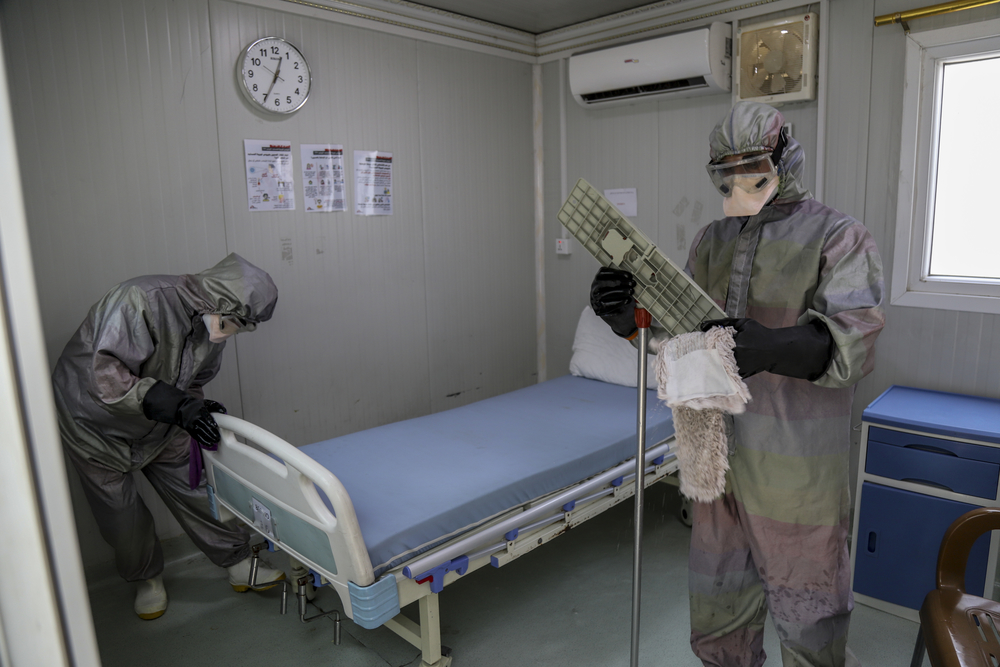
In order to ensure that health facilities are safe places for staff and patients and do not amplify the pandemic, MSF has implemented specific COVID-19 infection prevention and control measures in all our clinics and hospitals, and has supported health authorities in many countries to do the same in their facilities.
“In many places where we work, the MSF hospital or clinic might be a community’s only option for essential healthcare for hundreds of kilometres,” says Kate White. “People need to be able to trust that when they come to us – whether they are unwell with COVID-19, want to get care for their child with diarrhoea or malaria, or safely deliver their baby – they won’t come to more harm than if they hadn’t come to us in the first place.”
Beyond the hospital walls
At the same time, MSF teams have been looking beyond the hospital walls and adapting their medical activities to the specific needs of the communities where we work. While COVID-19 is certainly on almost everyone’s mind, it may not necessarily be the top priority health issue in every community.
“A cookie-cutter approach won’t work in this pandemic,” says Kate White. “We have to engage with communities to understand what their concerns are and adjust our activities in ways that both meet their most pressing health needs and simultaneously reduce the risks of COVID-19 transmission. It’s pointless if we try to roll out a perfect COVID-19 service, but it’s actually peak malaria or malnutrition season and that’s the main cause of sickness or death in that community.”
Some insurmountable challenges
Unfortunately, in some cases the challenges to continue providing care are currently insurmountable. In Syria, El Salvador, Malaysia and Mexico, teams have had to temporarily reduce or suspend mobile clinic activities; in Iraq, we have halted admissions of new patients into the non-communicable diseases program; in Monrovia, Liberia, we were forced to suspend paediatric surgeries due to staffing shortages caused by travel restrictions; in Pakistan we have suspended cutaneous leishmaniasis consultations in Balochistan and Khyber Pakhtunkhwa, as well as temporarily closed a maternity hospital in Peshawar; and in Zamfara, Nigeria we have temporarily closed most of our activities responding to lead poisoning.
With such uncertainty about our future capacity to guarantee a consistent supply of international staff and medical supplies, including personal protective equipment (PPE), all new planned initiatives have been put on hold. This includes the opening of a new maternity and paediatric facility in Qanawis, Yemen, where women and children continue to suffer the impact of an intense conflict.
Finding creative solutions
Around the world, MSF teams have been trying to find creative ways to keep healthcare accessible and to support frontline healthcare workers to care for their communities. There have been some remarkable initiatives, from increasing the availability of telemedicine, to providing online infection prevention and control trainings for care home workers, to running health promotion campaigns on social media, to managing WhatsApp groups of traditional healers.
We have reduced by half the recommended number of antenatal consultations for pregnant women to have in our clinics. In our maternal health projects in countries including Nigeria, DRC, Sierra Leone and Bangladesh, we are ensuring that women can still receive the care they need by engaging with trusted people in their communities – such as local health workers and traditional birth attendants – to identify when a woman needs to go to hospital because of complications.
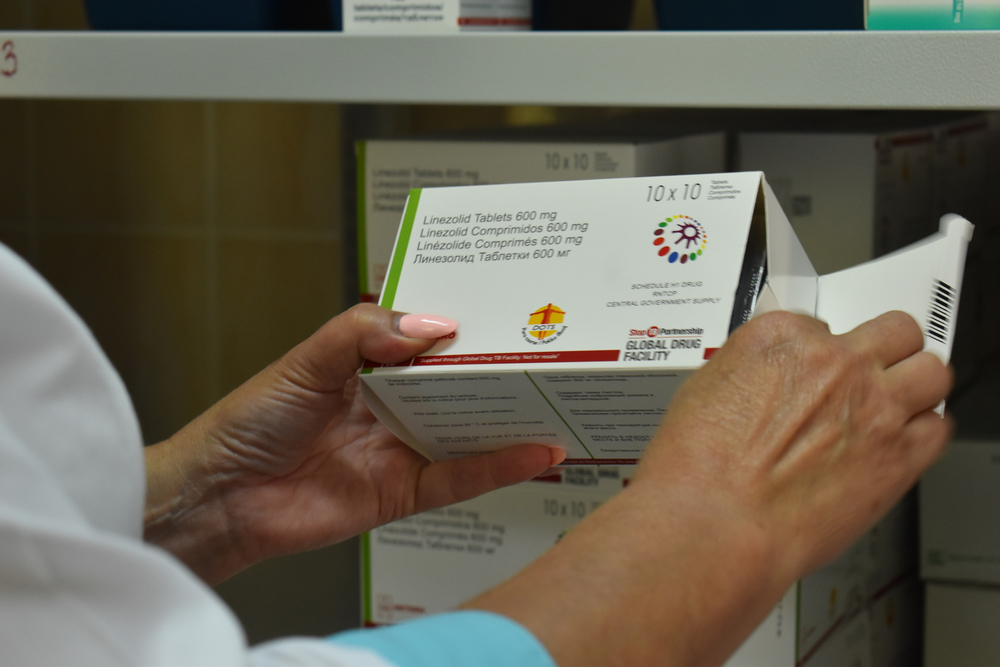
In our HIV, tuberculosis, hepatitis C and non-communicable disease projects in countries as diverse as South Africa, Ukraine, Pakistan and Cambodia, we have reduced routine consultations and distributed essential drugs to patients for longer periods (one to six months depending on the person’s health condition) so that they do not have to visit a health facility as often. At the same time, we are ensuring that patients receive follow-up through phone consultations, messaging apps and peer support networks.
Among the most at-risk for COVID-19 complications are people with underlying lung disease such as multidrug- resistant tuberculosis (MDR-TB). In Eswatini, the MSF team is reducing the risks for these vulnerable patients by bringing care closer to their homes and limiting unnecessary journeys by public transport to health centres. The majority of MSF’s 40 patients with MDR-TB are now using ‘video observed therapy’. MSF has given smartphones to patients so they can film themselves taking their medication and send the video to be checked by a nurse.
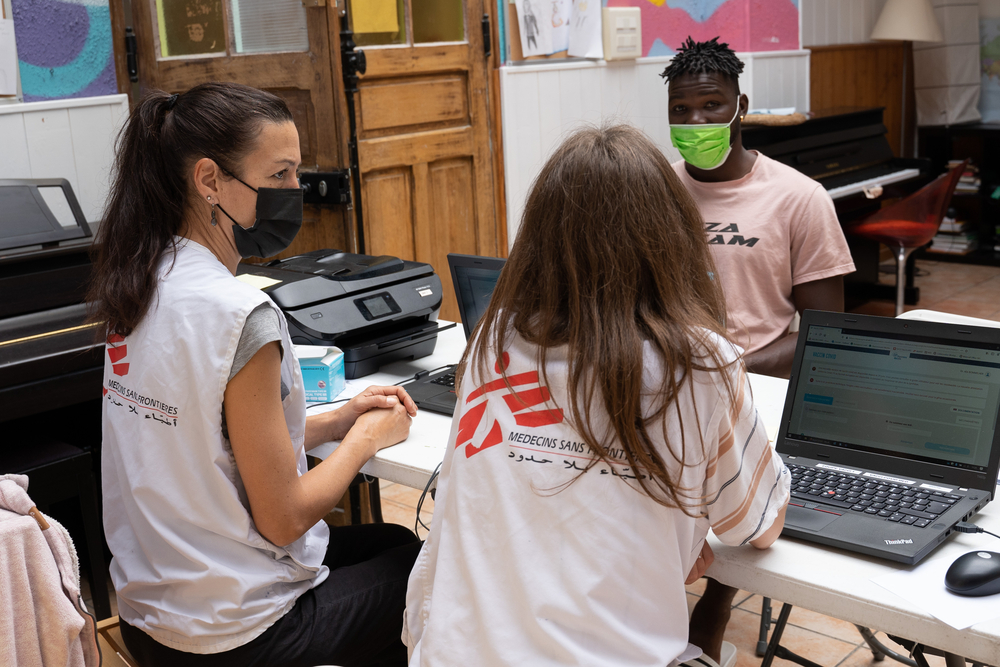
Meanwhile, many of MSF’s mental health services, including in El Salvador, Palestine and India, now offer telephone hotlines for existing and new patients, while counsellors and psychologists are providing consultations by phone. In Kashmir, where the COVID-19 lockdown has prevented MSF teams from running in-person mental health clinics, clinical psychologist Ajaz Ahmad Sofi says phone counselling has actually opened up the service to many more people. “Many of my new patients say that they have been avoiding visiting a counsellor because of a fear of being seen by relatives, neighbours or friends around the clinic. So while the lockdown has made lives much harder, in a way it has enabled more people to seek help, while allowing us to continue to provide a much needed medical service.”